
Hip injections. Is there a need for Ultrasound Guidance?
Many will have heard of steroid injections often in relation to musculoskeletal disorders. Many people know someone who has received a steroid injection for an osteoarthritic knee, a frozen shoulder or for any other musculoskeletal condition.
Fewer people might have heard of Hyaluronic Acid injections and maybe still fewer might have heard of Hydrodistension injections.
In this blog a brief summary into various type of injections such as hip, Steroid, Hyaluronic acid and Hydrodistension and their benefits. Also a brief summary of the differences between these injections option and indicate when they are likely to be most beneficial.
STEROID INJECTIONS
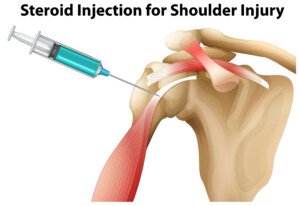
Steroid Injection for Shoulder Injury illustration
Often times patients are referred by their GP for a steroid injection when their shoulder, knee or whatever other joint or soft tissue problem they might be suffering with, is persistent, causing a lot of pain and is not responding to the usual first line treatments such as: relative rest, Non steroidal Anti-inflammatory drugs (NSAIDs) and or exercise therapy +/- physiotherapy.
Steroid injections when given appropriately are generally very safe and cause very little side effects. Please see our steroid information leaflet for some more information on steroid injections and their risks and side effects.
Steroid injections for musculoskeletal conditions should not to be confused with oral steroid (steroid pills) treatment. Usually the negative reports one hears about steroids refer to the side-effects associated with long term (usually oral) systemic steroid therapy (steroid pills). This tends to be for chronic conditions. For doctors to decide that the benefits outweigh the significant risks and side effects associated with long term steroid therapy it usually reflects the seriousness of the conditions that these people might be taking it for.
IN WHAT SITUATION IS A STEROID INJECTION MOST BENEFICIAL ?
Corticosteroids are synthetic drugs that resemble cortisol, a hormone that you produce in your adrenal glands. Corticosteroids have powerful anti-inflammatory effects. As a rule steroid injections are most useful for conditions where the pain, caused by a musculoskeletal condition, is a dominating feature and where there is a big impact on functional activities. Injections allow for an optimum dosage to a specific area of the body. Steroid injections tend to give pain relief relatively quickly, usually within one week following administration. Note that these are not the same drugs that some athletes use (illegally) to gain muscle strength.
HYALURONIC ACID INJECTIONS

Hyaluronic acid injections are also called viscosupplementation injections. Hyaluronic acid injections are most commonly used to treat symptoms of symptoms of knee osteoarthritis. Hyaluronic acid is an important component of the joint fluid in healthy joints, but is found in lower concentrations in osteoarthritic joints. By adding hyaluronic acid to the existing joint fluid the aim is to facilitate better joint movement, reduce pain and maybe slow down the progression of osteoarthritis.
IN WHAT SITUATION IS A HYALURONIC INJECTION MOST BENEFICIAL ?
Often good candidates for viscosupplementation are those with osteoarthritis who have failed to improve with other non-surgical treatments including steroid injections. Steroid injections can only be repeated for a limited number of times due to their potential side-effects. So regardless of the benefits of steroid injections hyaluronic acid injection might be a more suitable alternative in these circumstances.
Generally people who benefit from hyaluronic acid injections are active people for whom good movement in their joints is important. They should not be in severe acute pain as hyaluronic acid does not have the strong anti-inflammatory effects of a steroid injection and therefore might not provide enough pain relief in these more acute states.
Hyaluronic acid gives the joint fluid its viscous, slippery qualit
y, which enables the bones’ cartilage-covered surfaces to glide against each other, thereby reducing joint friction. It adds cushion to protect joints during impact (e.g. weight-bearing activity).
joints have lower concentrations of hyaluronic acid in their joint fluid than healthy joints, and therefore have less protection against joint friction and impact.
By injecting a synthetically made hyaluronanic acid into the knee the aim is to temporarily lubricate the knee joint, thereby decreasing pain improving function and hopefully slowing the degeneration process.
HYDRODISTENSION INJECTIONS

Hydrodistension or High Volume injections are performed under ultrasound guidance with the aim of precisely depositing anti-inflammatory steroid, local anaesthetic and saline to give pain relief whilst also deliberately stretching the lining of the joint (joint capsule). This procedure is increasingly used in the treatment of ‘frozen shoulder’ (adhesive capsulitis) and has been shown to be effective in the majority of patients by giving pain relief and also helping them to regain movement. These injections can give rapid and effective reduction in pain and inflammation; however, improvements are usually temporary. As with all medicines, some people may experience side effects.
IN WHAT SITUATION IS A HYDRODISTENSION INJECTION MOST BENEFICIAL ?
Clinically hydrodistension appears to be most useful in frozen shoulders where restriction rather than pain is the most dominant feature. As the injected volume is higher the procedure is likely to be slightly more uncomfortable when compared with a “normal” steroid injection under ultrasound guidance. This makes the procedure a good choice in “stiffness dominated” frozen shoulders.
Some research (Yoon et al. 2016) appears to support the above notion. Their study showed that hydrodistension plus steroid resulted in a bigger reduction in pain and a greater improvement of shoulder movement when compared to steroid injection alone in the first 3 months post injection. However patients in this study due to inclusion criteria were more likely to be in the more chronic stage (froze stage) of frozen shoulder when pain levels are reduced and the dominant problem is restriction of movement.
No such differences have been shown in other studies which included patients in the more acute earlier stages of frozen shoulder (Sharma, 2016; Lee, 2016). This might suggest that hydrodistension is more effective in those with significant shoulder stiffness but who are not in severe pain. More research is needed to evaluate this further.
References:
Lee, D.H., Yoon, S.H., Lee, M.Y., Kwack, K.S. and Rah, U.W., 2017. Capsule-Preserving Hydrodilatation With Corticosteroid Versus Corticosteroid Injection Alone in Refractory Adhesive Capsulitis of Shoulder: A Randomized Controlled Trial. Archives of physical medicine and rehabilitation, 98(5), pp.815-821.
Sharma, S.P., Bærheim, A., Moe-Nilssen, R. and Kvåle, A., 2016. Adhesive capsulitis of the shoulder, treatment with corticosteroid, corticosteroid with distension or treatment-as-usual; a randomised controlled trial in primary care. BMC musculoskeletal disorders, 17(1), p.232. Yoon, J.P., Chung, S.W., Kim, J.E., Kim, H.S., Lee, H.J., Jeong, W.J., Oh, K.S., Lee, D.O., Seo, A. and Kim, Y., 2016. Intra-articular injection, subacromial injection, and hydrodilatation for primary frozen shoulder: a randomized clinical trial. Journal of shoulder and elbow surgery, 25(3), pp.376-383.BLOGOG




.ashx?h=200&iar=0&mh=360&mw=520&w=200&hash=858D8DD88068FECC46AEA9F4BB0D4AB9)
